Just as our #PhysEd peers battle the old image of gym teachers, climbing ropes, playing dodgeball and bullying students, we too as health teachers have to push back against the perception that others have of what it is exactly that we do. I reached out to teachers to ask what misperceptions people have of health teachers so that I could address each one in turn.
We are Coach Carr from Mean Girls

This was the immediate response that came back to me, from a number of teachers and might be the most memorable portrayal of a health teacher on screen, if for all of the wrong reasons.
Don’t have sex, because you will get pregnant and die! Don’t have sex in the missionary position, don’t have sex standing up, just don’t do it, OK, promise? OK, now everybody take some rubbers.
First concern we should have with this is that clearly Coach Carr is a Coach and undoubtedly not a qualified health teacher. While historically health class hasn’t always been taught by a teacher with a health endorsement, best practice in health education includes having certified and/or highly trained health educators teaching health at all levels. Today’s health teachers should be fully certified and provided with regular professional development that allows them to improve their craft. If, like Coach Carr, you want to improve your teaching of Sex Ed, you should check out the Professional Learning Standards for Sex Education (PLSSE) aligning with theNational Sexuality Education Standards and theNational Teacher Preparation Standards for Sexuality Education, they include an assessment tool to help individuals, schools and organizations assess their competencies and identify needs for professional development.
Coach Carr also demonstrates another misconception of health teachers – that they are most effective when they use scare tactics – sharing scary stories, showing the most gruesome of photographs or the infamous “this is your brain on drugs” public service announcement.
Scare tactics often show extremes that will never be experienced by most people. Think of STI’s and the fact that the most common (and perhaps scariest) symptom is no symptoms at all. Fear might work with those individuals that are equipped with the skills needed to make behavioral change, but what use is a “Just Say No” campaign without equipping students with the ability to say no effectively? Students look to teachers to impart education, not scare and stigmatize them and their behaviors. The best health classrooms are the ones that are attending to the National Health Education Standards, establishing, promoting and supporting health-enhancing behaviors for students in all grade levels.
We are still showing THAT Video
I’m not sure exactly what THAT video was but I’m guessing it might have involved childbirth, on a bad quality VHS cassette. There is a popular Facebook group for Health teachers in which some great information is shared, but a common plea for advice is a teacher seeking a video suggestion to show in the classroom.
Brian Griffith wrote a great #slowchathealth blog post on the topic of integrating videos into the health classroom. A stand out quote was
Unfortunately some people use videos to keep them from having to teach. More than likely, those teachers aren’t reading blogs about teaching, they’re reading the sports page while teaching.
Brian shares wonderful ideas and hits the nail on the head when it comes to effective use of videos in the classroom. Earlier in my career I’ve been guilty of showing a full movie before and tenuously justifying it – Ferris Bueller’s Day Off to look for stressors and coping strategies!?! Thankfully with experience, and confidence in my teaching, I am more aware of when, and how much of a movie I should show to my students.
Our lessons are boring
No lesson should be boring in this day and age, and hopefully we have moved away from opening up a health book, reading the materials and completing the associated packet. Teaching health is a fantastic opportunity to encourage our students to consider their health and that of others. With increased pressure on academic scheduling it’s important that health educators get the most out of their time in the classroom and I have previously shared engaging ideas that should have students running to your class, eager to learn.
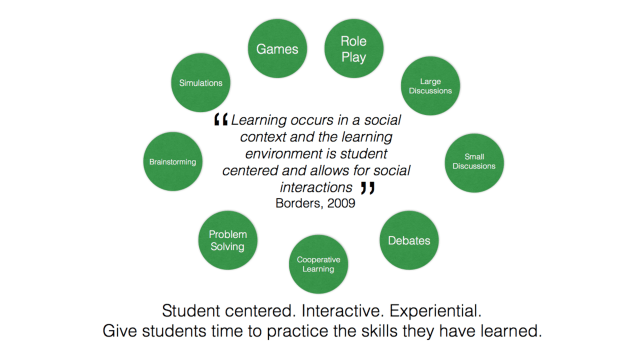
Students are the most important person in the room and they should be placed in the centre of the classroom experience. Survey your students and ask them what they want to do in health class and they’ll tell you that they want to interact with their peers. The image below suggests just some of the classroom activities you can incorporate as you make the move away from being the ‘sage on the stage’ to being the ‘guide on the side’.
2019 National Health Teacher of the Year Scott Todnem wrote a great blog post in which he shared his ‘Three Simple Things’ that he uses to energize his students.
All we teach is Sex, Drugs and Rock and Roll
No, although I do have friends who think that that is all that we teach. We are so much more than the varied content that we teach – and that content will vary from school to school based on the health needs of that particular community. By accessing Youth Risk Behavior Survey data we can identify the health behaviors that are most problematic among our young people and incorporate lessons on those topics while still teaching valuable health skills.
Skills Based Health is all about Social Emotional Learning, managing emotions, setting and achieving behavioral goals, showing empathy for others, establishing and maintaining positive relationships, and making responsible health decisions.
Many years ago a student said the following in one of my lessons.

This isn’t your mom or dad’s health class, this is an engaging space in which our students are being equipped with the skills needed for a lifetime of making well-informed decisions regarding their health, and advocating for the health of others along the way. The modern health class empowers our students and increases their self-efficacy.
Studies show that if we can get our students to believe that they have control over their health, then they are significantly more likely to be interested in the subject matter and eventually follow through with what they are taught in class. Conversely, low self-efficacy = low motivation = reduced follow through.
Increase self-efficacy and students will believe that they can set and achieve their goals. Increase self-efficacy and students will speak up when they see disparity and successfully advocate for others. Developing that positive mindset will embolden our students to make change in a world that desperately needs it.
We are the cause of teen behavior
In response to my asking of peoples perception of health teachers, ‘Kelly’ responded “don’t talk about (sex, pregnancy, suicide, depression, self inflicted violence, etc) because there will be a spike in it.” On the same platform, Carrie commented “If a kid is caught vaping it’s somehow my fault.”
Students will take risks – didn’t you when you were younger? I jumped out of a plane in my early twenties! Talking about risk behaviors will NOT encourage students to engage in that behavior, but leaving gaps in their knowledge by refusing to acknowledge or teach certain material will set our students up for failure. Failing to talk openly and candidly about topics such as sex can only lead to confusion and stigma.
The perfect example is the argument against ‘abstinence only until marriage’ (AOUM) sex education. By failing to give our students complete and medically accurate information we are doing them more harm than good. When those students engage in sex, they are less likely to use condoms or other forms of contraception which can prove to be problematic. What are we hoping to achieve by enforcing ‘no sex before marriage’ rules when typically Americans are increasingly getting married later, some don’t get married, and some are unable to get married. The average age for initiating sexual activity remains around 17 or 18 and has done so since the early 1990s. According to the Guttmacher Institute “considerable scientific evidence accumulated over the past 20 years has found that AOUM programs are not effective at preventing pregnancy or STIs, nor do they have a positive impact on age at first sexual intercourse, number of sexual partners or other behaviors.”
*Look out for Sexual Risk Avoidance (SRA) curricula which are AOUM under another name.
Why aren’t we solving teen behavior
As soon as a health concern reaches the media, all eyes turn towards health teachers. “Kids are eating Tide Pods? Why aren’t health teachers teaching them not to do this?”
Knee-jerk reactions will never go away and unfortunately some stake holders think that throwing another health behavior in our laps is the easiest way to ‘deal’ with a problem and pacify concerned parents.
The drug of choice seems to change quicker than the time it takes to rewrite a curriculum – see below.
Thankfully one of the many benefits of skills-based health is that content areas can be woven into our teaching of health skills. Once you have identified the health behavior you wish to address, you can select the skill and performance indicators you wish to teach before matching them up with the topic that you wish to cover. If you have identified that kratom use is a concern in your area then perhaps Accessing Valid and Reliable Information on the drug will be useful before you apply your Interpersonal Communication, practising refusal skills.
As health teachers, we should all be working towards addressing any of the common misperceptions that people have of us. We are all on a journey towards becoming master teachers and once we are confident in our own ability we should look to help those who have further to travel on their teaching journey.
Awesome documents for the inspired health educator include:
The Essential Components of Health Education from SHAPE America
The Whole School, Whole Community, Whole Child Model from ASHA
Suggested Job Interview Questions for Prospective Health Education Teachers from SHAPE America
This blog post was one, of many, that inspired me and helped shape the message of my October 2019 TEDx talk:
